
Hyperthyroidism Workup

Approach Considerations
The most reliable screening measure of thyroid function is TSH level. TSH levels usually are suppressed to immeasurable levels (< 0.05 Â IU/mL) in thyrotoxicosis. Third-generation TSH assays are recommended for screening purposes.
The most specific autoantibody test for autoimmune thyroiditis is an enzyme-linked immunosorbent assay (ELISA) test for anti-TPO antibody.
Hyperthyroidism in older patients often presents with atrial arrhythmias or CHF. Electrocardiography is recommended if an irregular heart rate or CHF is noted upon examination.
TSH and Thyroid Hormone Levels
Although measurement of the TSH level is the most reliable screening method for assessing thyroid function, the degree of thyrotoxicosis cannot be estimated easily in this way; thyrotoxicosis must instead be measured using an assay of thyroid hormone levels in the plasma. Thyroid hormone circulates as T3Â and T4, with 99% bound to protein.
Only the free, unbound thyroid hormone is biologically active. T3Â is 20-100 times more biologically active than T4. Of patients with thyrotoxicosis, 5% have only elevated T3Â levels. Therefore, measuring FT4Â (and FT3, Â if FT4Â levels are normal) is recommended in patients with suspected thyrotoxicosis when TSH is low.
Many laboratories do not measure free FT4Â directly, instead using a calculation to estimate the FT4Â levels. The free thyroxine index (FTI) is equal to total T4Â multiplied by the correction for thyroid hormone binding, such as the thyroid hormone ? binding ratio (THBR) or T3Â resin uptake [T3Â RU]). A similar calculation can be used with total T3.
Subclinical hyperthyroidism is defined as a suppressed TSH level (< 0.5 ?U/mL in many laboratories) in combination with serum concentrations of T3and T4Â that are within the reference range.
Other Laboratory Tests
As previously mentioned, the most specific autoantibody test for autoimmune thyroiditis is an ELISA test for anti-TPO antibody. The titers usually are significantly elevated in the most common type of hyperthyroidism, Graves thyrotoxicosis, and usually are low or absent in toxic multinodular goiter and toxic adenoma. A significant number of healthy people without active thyroid disease have mildly positive TPO antibodies; thus, the test should not be performed for screening purposes.
TSI, if elevated, helps to establish the diagnosis of Graves disease. A positive anti-TG antibody test does not predict the development of thyroid dysfunction, so the test should not be used.
Scintigraphy
If the etiology of thyrotoxicosis is not clear after physical examination and other laboratory tests, it can be confirmed by a iodine-123 (123 I) uptake, as in the images below. Values are elevated in patients with Graves disease and toxic multinodular goiters. 123I and technetium-99m (99m Tc) can be used for thyroid scanning, which provides anatomic information on the type of goiter (eg, diffuse vs nodular). Scans essentially are pictures of the thyroid and do not necessarily confirm or refute the presence of hyperthyroidism per se; only123I uptake provides information in this area.
Graves disease is associated with diffuse enlargement of both thyroid lobes, with an elevated uptake. A toxic adenoma demonstrates a solitary hot nodule with suppression of function in the surrounding normal thyroid tissue. A toxic multinodular goiter demonstrates an enlarged thyroid with multiple nodules and areas of increased and decreased isotope uptake. (See the first 2 images below.) Subacute thyroiditis usually demonstrates very low123I isotope uptake. (See the third image below.)
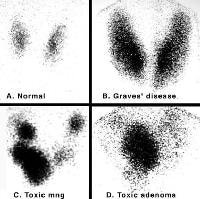 Iodine 123 (123I) nuclear scintigraphy: 123I scans of a normal thyroid gland (A) and common hyperthyroid conditions with elevated radioiodine uptake, including Graves disease (B), toxic multinodular
Iodine 123 (123I) nuclear scintigraphy: 123I scans of a normal thyroid gland (A) and common hyperthyroid conditions with elevated radioiodine uptake, including Graves disease (B), toxic multinodular

goiter (C), andtoxic adenoma (D).Scan in a patient with a toxic multinodular goiter. The 5-hour iodine uptake was elevated
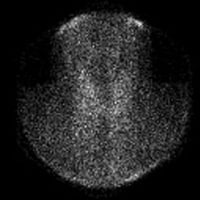
at 28%. Note the multiple foci of variably increased tracer uptake.Absence of iodine 123 (123I) radioactive iodine uptake in a patient with thyrotoxicosis and subacute painless or lymphocytic thyroiditis. Laboratory studies at the time of the scan demonstrated the following: thyroid-stimulating hormone (TSH), less than 0.06 mIU/mL; total thyroxine (T4), 21.2 mcg/dL (reference range, 4.5-11); total triiodothyronine (T3), 213 ng/dL (reference range, 90-180); T3-to-T4 ratio, 10; and erythrocyte sedimentation rate (ESR), 10 mm/h. The absence of thyroid uptake, the low T3-to-T4 ratio, and the low ESR confirm the diagnosis of subacute painless thyroiditis.
If a dominant nodule is found upon examination of a patient with thyrotoxicosis, obtain an123Â I thyroid scan to assure that the dominant nodule is functioning. If the nodule is cold, perform a biopsy on the nodule by fine-needle aspiration to exclude concomitant malignancy.
